

One in four U.S. adults — the equivalent of over 66 million Americans — report having used artificial intelligence tools or chatbots for physical or mental healthcare information or advice, according to new research released today from the West Health-Gallup Center on Healthcare in America. Rather than replacing traditional care, more than half say they turn to AI to supplement their healthcare experiences, using the technology before or after seeing a doctor.
The findings are based on a nationally representative survey of more than 5,500 U.S. adults conducted from October through December 2025.
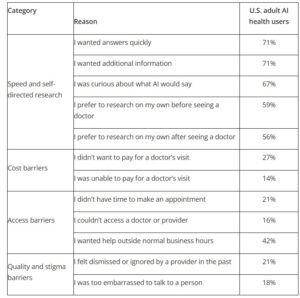
In the past 30 days, did you use an AI tool or chatbot for health-related information or advice for any of the following reasons?
% Yes, among adults who have used AI tools or chatbots for health-related information or advice in the past 30 days.

Note. Categories are for descriptive purposes only and were not shown on the survey.
Among Americans who have used AI for health-related information or advice in the past 30 days, the most frequently cited motivations are wanting answers quickly (71%) and wanting additional information (71%). Nearly seven in 10 (67%) say they were curious about what AI would say, and roughly six in 10 report using AI to do research on their own before (59%) or after (56%) seeing a doctor.
Regardless of the reason, almost half (46%) of Americans who used AI for healthcare information say the AI tool or chatbot made them feel more confident talking with or asking questions of a provider. Others say it helped them identify issues earlier (22%) or avoid unnecessary medical tests or procedures (19%).
“Artificial intelligence is already reshaping how Americans seek health information, make decisions and engage with providers, and health systems must keep pace,” said Tim Lash, President, West Health Policy Center, a nonprofit and nonpartisan organization focused on aging and healthcare affordability. “The risk isn’t that AI is moving too fast — it’s that health systems may move too slowly to guide its use in healthcare responsibly.”
A Smaller Share Turn to AI in Place of a Provider
While self-directed research is the primary driver of AI health use, a smaller but notable share of recent users report turning to AI instead of seeing a healthcare provider, particularly when faced with cost, access or quality barriers. Among recent AI health users, 27% say they didn’t want to pay for a doctor’s visit and 14% say they were unable to pay. One in five (21%) say they didn’t have time to make an appointment, and 16% say they couldn’t access a doctor or provider. Another 21% say they felt dismissed or ignored by a provider in the past, and 18% say they were too embarrassed to talk to a person.
In the past 30 days, did you use an AI tool or chatbot for health-related information or advice for any of the following reasons?
% Yes, among adults who have used AI for health-related information and advice in the past 30 days
| Household Income | % Yes, Among adults who have used AI for health-related information and advice in the past 30 days |
| <$24k | 32% |
| $24k – <$48k | 21% |
| $48k – <$90k | 14% |
| $90k – <$120k | 9% |
| $120k – <$180k | 8% |
| $180k+ | 2% |
Among recent AI health users, 84% still saw a healthcare provider, but 14% report not seeing a provider they otherwise would have seen because of information or advice they received from AI. When projected to the full U.S. adult population, this represents roughly 14 million Americans who did not see a provider after receiving AI-generated health information.
Trust in that AI-generated health information, however, remains divided. Among those who consulted it in the past 30 days, roughly one-third say they trust it (33%), one-third neither trust nor distrust it (33%), and about one-third distrust it (34%). However, only 4% say they strongly trust the accuracy, indicating that many Americans are making healthcare decisions based on AI-generated information without full confidence in its accuracy.
About one in 10 (11%) who report using AI for health information or advice in the past 30 days say that AI recommended healthcare information or advice they believed was unsafe.
“This data indicates that while some Americans may be using artificial intelligence as a substitute for going to the doctor’s office, many see it as a tool to complement their healthcare, helping them understand symptoms they might be feeling and clarify any diagnosis they receive from their doctors,” said Joe Daly, Global Managing Partner at Gallup.
Motivations Vary by Age and Income
While information-seeking is the dominant reason Americans turn to AI for health purposes, use patterns differ by demographics. Younger adults are more likely than older adults to use AI for self-directed research — 69% of adults aged 18 to 29 say they do research before seeing a doctor, compared with 43% of those 65 and older.
Income differences are most visible in barrier-driven motivations. Among adults earning less than $24,000 annually, 32% say they used AI because they could not pay for a doctor’s visit, compared with just 2% among those earning $180,000 or more.
Everyday Health Questions Top the List of AI Use Cases
Americans who used AI for health information or advice in the past 30 days most often report using it to gather information about everyday health concerns, including physical symptoms (58%) and nutrition or exercise (59%). But AI use extends beyond symptom-checking — Americans who used AI in the past 30 days also report using AI to understand medication side effects (46%), interpret medical information (44%), or research a diagnosis or medical condition (38%). Nearly one in four (24%) report using AI to explore mental health or emotional concerns.
Also Read:
Doctors Say Start Screening Cholesterol Earlier. Here’s What Changed
A Heart Test Could Reveal Hidden Fracture Risk in Women After Menopause: Study





")
")
 and colleagues visit a WHO-supported health centre providing care to the population around Goma. (file)")

